

Incontinence is involuntary loss of urine. Urinary incontinence is a significant health problem with considerable social and economical impact on individual and society.In young women, the prevalence of incontinence is usually low; but prevalence peaks around menopause, with steady rise thereafter into later life. Although the prevalence of stress and mixed (stress and urge ) incontinence is higher than urge incontinence, the latter is more likely to require treatment.
Signs and Symptoms
In women moderate and severe bother have a prevalence ranging from about 3% to17
Types of incontinence
- Continuous incontinence: loss of urine loss at all times and in all position
- Stress incontinence: Sudden leakage of urine with coughing, sneezing or exercise. It is commonly seen in women after childbirth or menopause due to loss of support.
- Urge incontinence: loss of urine is precede by strong urge to pass urine
- Overflow incontinence or paradoxical incontinence: secondary to urinary retention or incomplete emptying of urine. It is paradoxical because incontinence is cured by relief of bladder outflow obstruction.
- Nocturnal Enuresis: is incontinence that occurs during sleep.Normal in child up to age of three. Seen in 1% of children at the age of 15. Vast majority will be found to have no significant urologic abnormality.
Stress Incontinence
Stress incontinence is sudden leakage of urine with coughing, sneezing or exercise. It is commomly seen in women after childbirth or menopause. Commonly due to weakness of pelvic floor muscle, urinary sphincter (valve) of combinatoin of both.
Treatment
- Pelvic floor exercise
Pelvic floor exercise is done to strengthen the pelvic floor muscles. It has to be done regularly and several times a day. It takes only few minutes and results are expected only after 6 months if they are done regularly. Pelvic floor exercises along with medications have produced good results in patients with mild to moderate incontinence.
 |
 |
|
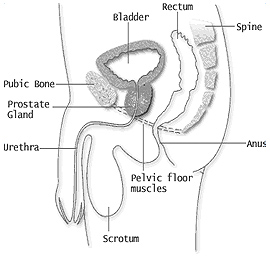
Pelvic Floor in Men
|
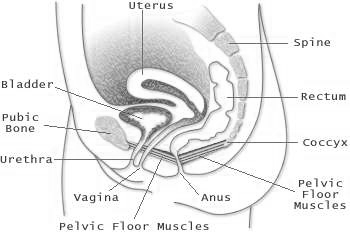
Pelvic Floor in Women
|
- Medications
- Surgical Treatment (Slings)

Slings
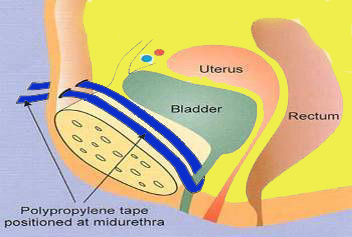
- Pubovaginal and Suburethral slings: This procedure involves placing a band of sling material directly under the bladderneck or mid urethra, which acts as a physical support to prevent bladder neck and urethral descent during physical activity. The sling may also augment the resting urethral closure pressure with increases in intra-abdominal pressure. Autologous tissue used include rectus fascia, fascia lata. Sling implants used include Monarc, IVS, SPARC, TVTO.
- Currently Mid urethral sling are not advocated as first line management for the risk of long term complications
- Colposuspension and Autologous slings are preferred.
- Intravesical Injection of Botox is treatment choice for intractable overactive bladder in patient with failure of medical management.
Overactive Bladder (OAB)
Overactive bladder (OAB) is a urological condition defined by International Continence Society as set of symptoms with urgency, with or without urge incontinence, usually with frequency and nocturia.
Normal physiology
Normally, the bladder muscle contracts and relaxes in response to the volume of urine in the bladder and the initiation of urination.In people with an overactive bladder (OAB),the bladder muscle contracts spastically, sometimes without a known cause, which results in sustained, high bladder pressure and the urgent need to urinate (called urgency). People with OAB often experience urgency at inconvenient and unpredictable times and sometimes loses control before reaching a toilet. Thus, overactive bladder interferes with work, daily routine, intimacy and sexual function; causes embarrassment; and can diminish self-esteem and quality of life.
Urination (micturition) involves processes within the urinary tract and the brain. The slight need to urinate is sensed when urine volume reaches about one-half of the bladder’s capacity. The brain suppresses this need until a person initiates urination
Once urination has been initiated, the nervous system signals the detrusor muscle to contract into a funnel shape and expel urine. Pressure in the bladder increases and the detrusor muscle remains contracted until the bladder empties. Once empty, pressure falls and the bladder relaxes and resumes its normal shape.
Overactive bladder affects men and women equally.
Signs and Symptoms
There are three symptoms associated with an overactive bladder:
- Frequency (frequent urination)
- Urgency (urgent need to urinate)
- Urge incontinence (strong need to urinate followed by leaking or involuntary and complete voiding)
Diagnosis
- Medical history
- Voiding diary
- Physical examination
- Urodynamic study
Treatment
Treatment may include one or more of the following:
- Lifestyle modification (fluid restriction, avoidance of coffee and tea),
- Bladder retraining ( patient uses this timetable to plan when to empty the bladder to avoid accidental leakage).
- Medications
- Sacral nerve stimulation (implanted neurostimulatory system sends mild electrical pulses to the sacral nerve, the nerve near the tailbone that influences bladder control muscles. Stimulation of this nerve may relieve the symptoms related to urge incontinence)
- Surgery like Intravesical botulinum toxin
- Surgical augmentation of the bladder